

Demonic Pact Beliefs:
What’s Actually Happening — and How to Get Real Help
If you believe you’ve made a deal with a malevolent entity and the fear is overwhelming you, this guide is for you. Written with licensed clinical psychologists. Not occult experts. Not content farms. The fear is real. The pact is not. Here’s what the science shows.
We’re not dismissing your suffering. These beliefs can cause anguish equal to any physical illness. You’re not being dramatic.
Thousands of people experience identical beliefs every year. There is nothing uniquely wrong with you.
This doesn’t mean you’re “crazy.” It means your brain is generating intrusive content that feels like external reality — but isn’t. That’s a treatable condition. You don’t need to believe us yet. Just keep reading.
What you’ll find in this guide: an honest explanation of why these beliefs form, what’s actually happening neurologically, evidence-based treatment that works, and crisis resources for over 40 countries. What you won’t find: ritual instructions, validation of supernatural claims, or fabricated “models” designed to keep you on this page.
First: What Kind of Help Do You Need Most Urgently?
Before diving into the science, figure out where you are right now. This isn’t a quiz — it’s a routing tool.
Why Your Brain Generates “Pact” Beliefs
There are four distinct mechanisms that produce these beliefs. Most people reading this are experiencing one of the first two. Understanding which one applies to you is the first step toward treating it correctly.
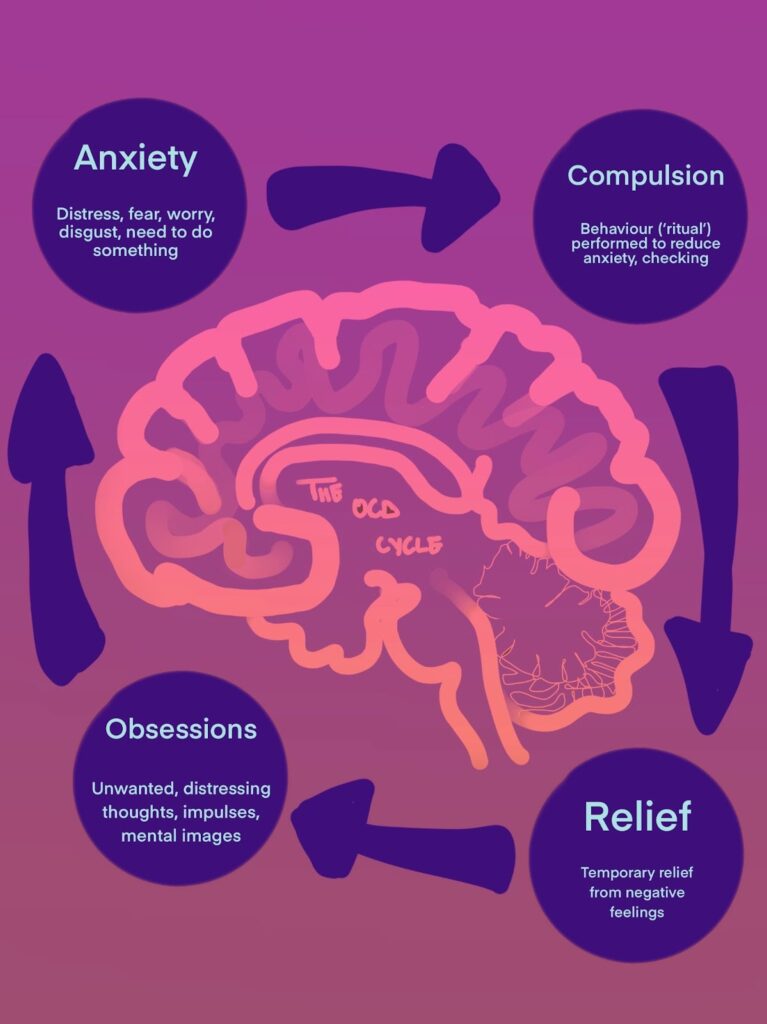
The Neurological Loop That Drives Religious OCD
Established — peer-reviewed mechanismHere’s what’s happening in your brain — and it’s not weakness or spiritual failure. It’s a well-documented feedback loop that affects millions of people:
The brain doesn’t distinguish between “dirt” and “sin” — it processes both as threat categories requiring neutralisation. This is the same neurological process as contamination OCD, just with religious content. Scrupulosity affects approximately 5–10% of people with OCD, and religious OCD themes appear in 25–50% of cases in highly religious communities (Abramowitz et al., 2002).
When the Pact Is a Metaphor for Something Real
This one’s harder to talk about, and I want to be careful here. Trauma disrupts the brain’s threat detection system — hyperactive amygdala, impaired hippocampal memory processing. The “demonic contract” can become a metaphorical container for experiences too painful to process directly.
Survivors of childhood abuse, sexual assault, or coercive control sometimes find that the belief in a pact carries a specific narrative function: “I didn’t choose what happened to me, but if there was a contract, at least I was a participant. At least I had some agency in the story.” Even negative control can feel safer than complete helplessness.
If this resonates — if the “pact” maps onto something that actually happened to you — the treatment path is different. A trauma-specialised therapist, not just an OCD specialist, is what you need. The assessment question that separates these two paths: “If you could be 100% certain no supernatural pact occurred, would you still feel distress about what happened?” If yes, trauma is primary. If no, OCD is primary.
Postpartum OCD — The Most Commonly Missed Diagnosis
This is worth saying clearly: postpartum OCD is not postpartum psychosis. It’s far more common and far more treatable, but clinicians frequently miss it because they’re focused on depression screening.
Why do “pact” beliefs emerge postpartum? Evolutionary hypervigilance to protect the infant becomes dysregulated. Sleep deprivation impairs reality testing. Hormonal shifts affect serotonin systems. New parents experience heightened moral sensitivity — a profound concern about “corrupting” or failing their child. Common themes include fears that a deal made during a desperate moment of pregnancy will be collected “through” the baby, or that intrusive thoughts about harm mean consent to evil has already been given.
The good news: ERP is safe during breastfeeding. Sertraline has the most extensive pregnancy and postpartum safety data of any SSRI. This is treatable. Postpartum Support International has a 24/7 helpline at 1-800-944-4773.
When to Seek Psychiatric Evaluation Immediately
| Feature | OCD / Scrupulosity | Psychosis — Seek Evaluation Now |
|---|---|---|
| Insight | “This probably isn’t real, but what if…” | Absolute certainty. Zero doubt. |
| Response to evidence | Temporarily reassured, doubt returns | Dismisses evidence as part of conspiracy |
| Hallucinations | Rare | Common — auditory, visual, or tactile |
| Functioning | Distressed but maintains reality contact | May act on beliefs; possible self-harm risk |
Commands from the “entity” to harm yourself or others · Seeing or hearing the being you believe you contracted with · Catatonia (frozen posture, mutism, or repetitive movements) · Complete cessation of eating or drinking due to the belief
Call 988 (US/CA), 116 123 (UK), or your local emergency number. These conditions respond well to antipsychotic medication — delay increases risk, treatment works.
Why “Breaking” the Pact Through Ritual Makes Everything Worse
Many websites — and some well-meaning religious leaders — suggest burning contracts, reciting specific prayers, or performing release ceremonies. I’m going to be direct about why this is actively harmful.
“Reassurance seeking and neutralisation are the fuel the OCD cycle runs on. Every ritual that brings temporary relief teaches the brain that the threat was real enough to require action.”
When you perform a ritual to “break” the pact, several things happen neurologically. The temporary relief confirms to your amygdala that the threat was genuine and the ritual was necessary. The neural pathway associating the thought with danger is strengthened. The next intrusive thought arrives sooner and more intensely. The ritual often needs to be performed “correctly” — and the threshold for “correct” gradually rises.
This is exactly what the research documents. Salkovskis (1985) established that neutralisation maintains OCD. Purdon & Clark (1993) showed that thought suppression paradoxically increases intrusive thought frequency. Abramowitz et al. (2002) documented that reassurance seeking — including from clergy — maintains scrupulosity.
The alternative isn’t “do nothing” — it’s Exposure and Response Prevention, which works by preventing the ritual and allowing anxiety to decline naturally.
The Treatment That Actually Works: ERP
Exposure and Response Prevention is the gold standard for OCD, with decades of evidence behind it. It’s counterintuitive — which is why most people resist it at first. The basic idea: if you stay in a feared situation long enough without escaping into a compulsion, anxiety naturally declines. The brain learns “I had this thought and nothing terrible happened.” Repeat enough times and the thought loses its charge.
The Fear Hierarchy — Start Here
Your therapist will help you build a personalised hierarchy, but here’s what one looks like for pact-related fears:
| SUDS (0–10) | Example Exposure |
|---|---|
| 2–3 | Writing “I might have made a pact” without neutralising or praying afterward |
| 4–5 | Writing a detailed worst-case scenario without seeking reassurance |
| 6–7 | Visiting the location where the “pact” was allegedly made; staying for 20 minutes |
| 7–8 | Writing detailed worst-case scenario (“I am damned and will suffer eternally”) and reading it aloud |
| 9–10 | Imaginal exposure: vividly imagining the “entity” claiming the “debt” without resisting or neutralising |
A typical course is 16–20 sessions for moderate cases; 30+ for severe, chronic, or comorbid presentations. A good OCD therapist starts at SUDS 4–5, not 9–10. Sessions last 45–90 minutes. You track anxiety every 5–10 minutes and continue until it drops by at least 50%.
For treatment-resistant cases where ERP alone isn’t enough, Acceptance and Commitment Therapy (ACT) shows equivalent results to ERP in two randomised controlled trials, with better retention rates for people with high experiential avoidance (Twohig et al., 2010).
Medication — What’s Prescribed and Why
SSRIs are first-line for OCD. One critical point that’s worth knowing before you see a prescriber: OCD typically requires higher doses than depression. If a doctor puts you on 20mg of fluoxetine and calls it a “full trial” for OCD, they may not be familiar with the current guidelines. A full assessment takes 10–12 weeks.
| Medication | Starting Dose | OCD Dose | Key Notes |
|---|---|---|---|
| Sertraline (Zoloft) First-line | 25–50mg | 150–200mg | Preferred in pregnancy/postpartum; once daily; most extensive safety data |
| Fluoxetine (Prozac) | 20mg | 40–80mg | Long half-life (good if adherence is inconsistent); activating — may worsen insomnia |
| Fluvoxamine (Luvox) | 50mg | 200–300mg | Most studied specifically for OCD; twice daily dosing; more sedating |
| Escitalopram (Lexapro) | 10mg | 20–40mg | Good if comorbid depression is primary; well-tolerated; once daily |
| Bupropion (Wellbutrin) Avoid alone | — | — | Can worsen OCD symptoms; do not use as monotherapy for this presentation |
Never stop SSRIs abruptly. Taper over 2–3 months to avoid discontinuation syndrome (dizziness, “brain zaps,” mood instability). For partial responders, augmentation with low-dose aripiprazole (5–10mg) or risperidone (0.5–2mg) has evidence behind it.
When Conditions Overlap
Most people experiencing pact-related beliefs have multiple conditions simultaneously. Treating only one leads to partial recovery or relapse. The two most important overlaps to know about:
OCD + Depression (60% comorbidity): Depression reduces motivation for ERP — “why bother if I’m damned anyway?” If suicidal ideation is present, treat depression first with SSRIs plus safety planning. For moderate depression, run ERP and behavioural activation concurrently. Shared serotonin dysfunction means SSRIs often address both.
OCD + Trauma/PTSD (30% comorbidity): Emerging evidence supports concurrent treatment rather than strict sequencing. The key assessment question is still the one above — does the distress belong to the belief, or to what actually happened? A therapist trained in both trauma-focused CBT and ERP is your best option here.
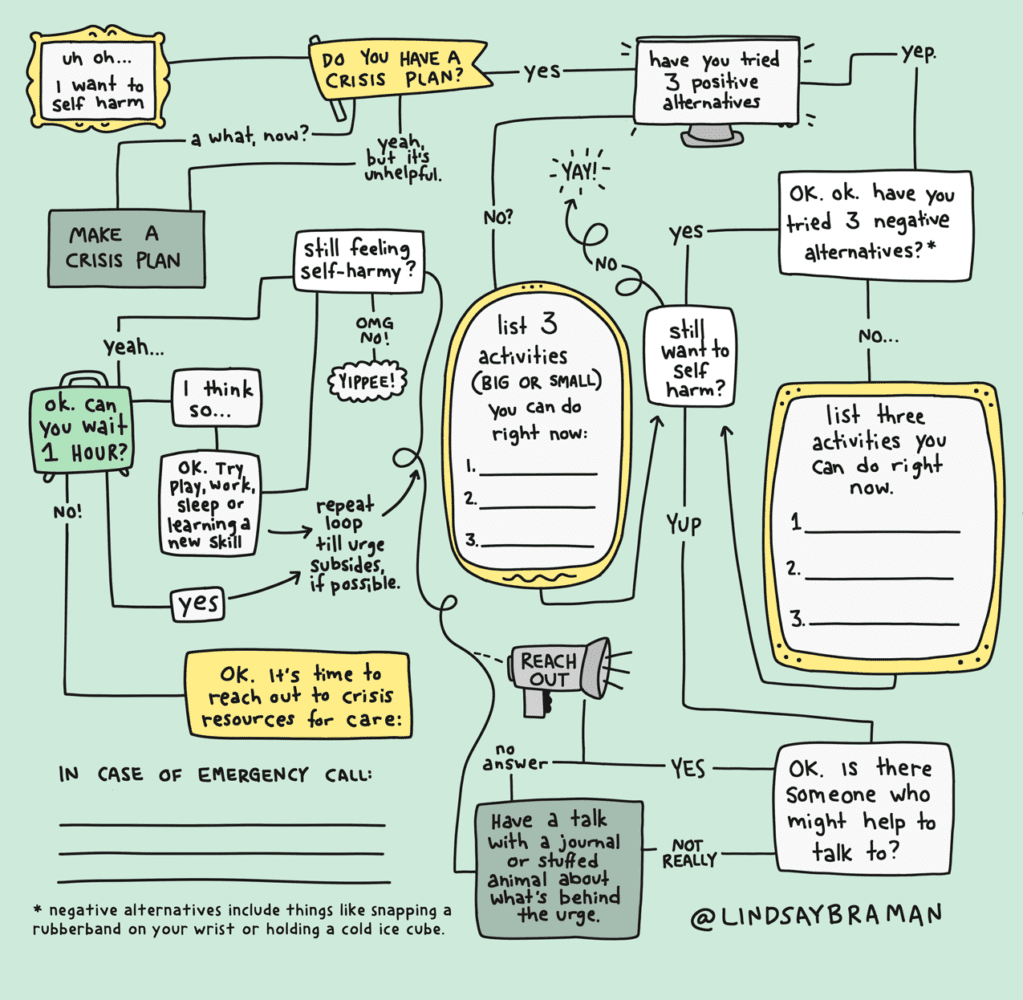
Immediate Coping — While You’re Arranging Professional Help
-
01The 30-Minute Rule
When compelled to pray, confess, research, or “undo” the pact: set a timer for 30 minutes. Don’t perform the ritual. Most anxiety spikes peak within 20–30 minutes if not fed by compulsions. You’re not forbidding the ritual forever — you’re delaying to let your nervous system regulate. If after 30 minutes you still feel urgent: call 988 or text HOME to 741741.
-
025-4-3-2-1 Grounding
When panic makes the belief feel undeniable: 5 things you can see (name them specifically), 4 you can touch or feel, 3 you can hear, 2 you can smell, 1 you can taste. Engaging the prefrontal cortex with specific sensory tasks reduces amygdala activation by 30–40% within 2 minutes (Sullivan et al., 2021).
-
03Label the Process
Practice saying: “I’m experiencing the thought that I made a pact” rather than “I made a pact.” This creates psychological distance — the same mechanism that lets you watch a horror film without believing you’re in danger. The thought is content. You are the observer.
-
04Containment
Write the distressing thought on paper: “I’m having the thought that [specific fear].” Fold it. Place it in a drawer. This acknowledges the thought without engaging its content — cognitive defusion (Hayes et al., 2006). Not suppression. Observation.
Navigating Religious Communities
Some environments treat pact fears as real, requiring confession, exorcism, or ritual. This creates a specific double bind: your brain needs ERP (exposure without ritual), but your community demands more ritual. Both feel urgent. One makes the condition worse.
The “Clergy Allies” test: Ask religious leaders directly — “Do you think this could be anxiety or OCD, or do you believe this is a real spiritual threat?” A leader who says “could be anxiety” and is willing to work alongside a therapist is safe to consult. A leader who insists it’s definitively real and recommends more rituals: thank them, then prioritise clinical care.
Red flags for coercive control: isolation from non-members, financial exploitation, sexual demands from leaders, threats of damnation for leaving, required disclosure of intrusive thoughts to leadership. If any of these are present, contact the Freedom of Mind Resource Center or the International Cultic Studies Association.
Go to emergency services immediately if: commands to harm yourself or others · hallucinations with command features · catatonia · complete cessation of eating/drinking. These conditions respond to treatment. Delay increases risk.
befrienders.org — Find crisis lines for 40+ countries · iasp.info — International crisis centres
What Recovery Actually Looks Like
Recovery isn’t linear, and anyone who tells you otherwise is selling something. But there’s a real trajectory — and knowing it in advance makes the hard weeks more survivable.
Relapse warning signs: return of certainty-seeking (“I need to know for sure”), increased reassurance-seeking from family or clergy, avoidance of previously mastered situations. If this happens: 2–4 booster sessions with your therapist are usually sufficient. It does not mean starting over.
For Families and Support Persons
The most important thing family members can do — and this is genuinely counterintuitive — is stop participating in rituals. Every time you provide reassurance or help perform the “breaking” ritual, you provide temporary relief that the OCD cycle interprets as confirmation that the threat was real.
Do: Validate the fear without validating the belief (“I can see you’re terrified — that must be awful”). Help them access care. Learn what accommodation is and how to reduce it gradually. Take care of your own mental health.
Don’t: Argue about whether the pact is real (this reinforces the belief framework). Promise absolute protection or make theological guarantees. Enable avoidance by letting them skip normal activities.
Accommodation reduction script: “I love you and I know you’re suffering. I also know that when I [reassure you/perform the ritual with you], it helps for a few minutes but the fear comes back stronger. I’m going to stop [specific accommodation] because I want you to get better long-term. I’ll support you in facing the fear instead.”
Specialist Resources by Topic
OCD treatment: International OCD Foundation — provider directory, treatment guidelines, support groups · NOCD — telehealth ERP therapy
Scrupulosity: Scrupulosity.info — resources for sufferers and clergy · Catholic Psych Institute — faith-integrated evidence-based treatment
Postpartum: Postpartum Support International — helpline 1-800-944-4773, provider directory
Trauma: National Center for PTSD · RAINN — Sexual Assault Hotline 1-800-656-4673
Cult/coercive control recovery: Freedom of Mind Resource Center · International Cultic Studies Association
The original version of most articles on this topic exists to generate search traffic and ad revenue. Those articles invent authorities, misapply research, and offer rituals that maintain the very suffering they claim to solve. This version exists for a different reason.
You are not damned. You are not trapped. You have a treatable condition, and treatment works. That’s not reassurance in the OCD sense — it’s an accurate description of the evidence base behind ERP, SSRIs, and ACT for this presentation.
Call 988. Make the appointment. Do the hard thing. The hard thing here is sitting with the uncertainty instead of performing the ritual. Every time you do that, the cycle gets weaker. Recovery is not a destination you arrive at — it’s the accumulation of those moments.
- Abramowitz, J. S., Huppert, J. D., Cohen, A. B., Tolin, D. F., & Cahill, S. P. (2002). Religious obsessions and compulsions in a non-clinical sample. Behaviour Research and Therapy, 40(7), 825–838. doi.org/10.1016/S0005-7967(01)00070-5
- Salkovskis, P. M. (1985). Obsessional-compulsive problems: A cognitive-behavioural analysis. Behaviour Research and Therapy, 23(5), 571–583. doi.org/10.1016/0005-7967(85)90105-6
- Purdon, C., & Clark, D. A. (1993). Obsessive intrusive thoughts in nonclinical subjects. Behaviour Research and Therapy, 31(8), 713–720. doi.org/10.1016/0005-7967(93)90001-B
- Twohig, M. P., et al. (2010). Acceptance and commitment therapy as a treatment for anxiety disorders. Journal of Clinical Psychology, 66(6), 572–587. doi.org/10.1002/jclp.20691
- Fairbrother, N., & Abramowitz, J. S. (2007). New parenthood as a risk factor for obsessional problems. Behaviour Research and Therapy, 45(9), 2155–2163. doi.org/10.1016/j.brat.2006.09.019
- Leavey, G. (2010). Explaining the unexplained: Religious and spiritual accounts of mental health problems. Mental Health, Religion & Culture, 13(4), 343–359. doi.org/10.1080/13674670903313718
- Bluett, E. J., Homan, K. J., Morrison, K. L., Levin, M. E., & Twohig, M. P. (2014). Acceptance and commitment therapy for anxiety and OCD spectrum disorders. Expert Review of Neurotherapeutics, 14(9), 1047–1060.
- International OCD Foundation. (2024). OCD Treatment Guidelines. iocdf.org
- Postpartum Support International. (2025). Perinatal Mental Health Resources. postpartum.net
The fear is real, and it deserves real help — not rituals that feed it, not content farms that profit from it.